Pyomyositis
| Pyomyositis | |
|---|---|
 | |
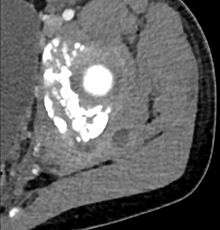
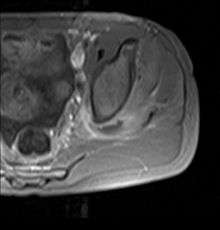
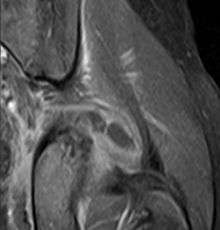
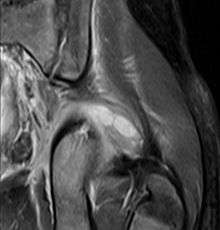
| Transverse T2 magnetic resonance imaging section through the hip region showing abscess collection in a patient with pyomyositis. | |
| Classification and external resources | |
| Specialty | rheumatology |
| ICD-10 | M60.0 |
| ICD-9-CM | 040.81, 728.0 |
| DiseasesDB | 29474 |
| MeSH | D052880 |
| Orphanet | 764 |
Pyomyositis, also known as tropical pyomyositis or myositis tropicans, is a bacterial infection of the skeletal muscles which results in a pus-filled abscess. Pyomyositis is most common in tropical areas but can also occur in temperate zones.

Epidemiology
Pyomyositis is most often caused by the bacterium Staphylococcus aureus.[1] The infection can affect any skeletal muscle, but most often infects the large muscle groups such as the quadriceps or gluteal muscles.[2][3][4]
Pyomyositis is mainly a disease of children and was first described by Scriba in 1885. Most patients are aged 2 to 5 years, but infection may occur in any age group.[5][6] Infection often follows minor trauma and is more common in the tropics, where it accounts for 4% of all hospital admissions. In temperate countries such as the US, pyomyositis was a rare condition (accounting for 1 in 3000 pediatric admissions), but has become more common since the appearance of the USA300 strain of MRSA.[2][3][4]
Treatment
The abscesses within the muscle must be drained surgically (not all patient require surgery if there is no abscess). Antibiotics are given for a minimum of three weeks to clear the infection.[2]
References
- ↑ Chauhan S, Jain S, Varma S, Chauhan SS (2004). "Tropical pyomyositis (myositis tropicans): current perspective". Postgrad Med J. 80 (943): 267–70. doi:10.1136/pgmj.2003.009274. PMC 1743005
 . PMID 15138315.
. PMID 15138315. - 1 2 3 Pannaraj PS, Hulten KG, Gonzalez BE, Mason EO Jr, Kaplan SL (2006). "Clin Infect Dis". Clinical Infectious Diseases. 43 (8): 953–60. doi:10.1086/507637. PMID 16983604.
- 1 2 Ovadia D, Ezra E, Ben-Sira L, et al. (2007). "Primary pyomyositis in children: a retrospective analysis of 11 cases". J Pediatr Orthop B. 16 (2): 153–159. doi:10.1097/BPB.0b013e3280140548. PMID 17273045.
- 1 2 Mitsionis GI, Manoudis GN, Lykissas MG, et al. (2009). "Pyomyositis in children: early diagnosis and treatment". J Pediatr Surg. 44 (11): 2173–178. doi:10.1016/j.jpedsurg.2009.02.053. PMID 19944229.
- ↑ Small LN, Ross JJ (2005). "Tropical and temperate pyomyositis". Infect Dis Clin North Am. 19 (4): 981–989. doi:10.1016/j.idc.2005.08.003.
- ↑ Taksande A, Vilhekar K, Gupta S (2009). "Primary pyomyositis in a child". Int J Infect Dis. 13 (4): e149–e151. doi:10.1016/j.ijid.2008.08.013. PMID 19013093.