Pseudoxanthoma elasticum
| Pseudoxanthoma elasticum | |
|---|---|
 | |
| Pseudoxanthoma elasticum of the posterior lateral neck. Note the yellowish slightly raised bumps characteristic of this condition. | |
| Classification and external resources | |
| Specialty | medical genetics |
| ICD-10 |
Q82.8 (ILDS Q82.81) |
| ICD-9-CM | 757.39 |
| OMIM | 264800 |
| DiseasesDB |
1088510894 |
| eMedicine | derm/359 oph/475 |
| Patient UK | Pseudoxanthoma elasticum |
| MeSH | D011561 |
Pseudoxanthoma elasticum (PXE), also known as Grönblad–Strandberg syndrome,[1] is a genetic disease that causes fragmentation and mineralization of elastic fibers in some tissues. The most common problems arise in the skin and eyes, and later in blood vessels in the form of premature atherosclerosis.[2] PXE is caused by autosomal recessive mutations in the ABCC6 gene on the short arm of chromosome 16 (16p13.1).[2][3]
Signs and symptoms
Usually, pseudoxanthoma elasticum affects the skin first, often in childhood but frequently later. Small, yellowish papular lesions form and cutaneous laxity mainly affects the neck, axillae (armpits), groin, and flexural creases (the inside parts of the elbows and knees). Skin may become lax and redundant. Many individuals have "oblique mental creases" (diagonal grooves of the chin).[2]
PXE first affects the retina through a dimpling of the Bruch membrane (a thin membrane separating the blood vessel-rich layer from the pigmented layer of the retina), that is only visible during ophthalmologic examinations. This is called peau d'orange (a French term meaning that the retina resembles the skin of an orange). Eventually the mineralization of the elastic fibers in the Bruch membrane create cracks (angioid streaks) that radiate out from the optic nerve. Angioid streaks themselves do not cause distortion of vision, even if they cross into the foveal area. This symptom is present almost all PXE patients and is usually noticed a few years after the onset of cutaneous lesions. These cracks may allow small blood vessels that were originally held back by Bruch's membrane to penetrate the retina. These blood vessels sometimes leak, and these retinal hemorrhages may lead to the loss of central vision. Vision loss is a major issue in many PXE patients.[2][3]
PXE may affect the gastrointestinal and cardiovascular systems. In the digestive tract, the principal symptom is gastrointestinal bleeding, usually from the stomach. This occurs in very small number of patients. In the circulatory system, intermittent claudication (leg pain during walking which resolves at rest) is a prominent feature, although at later stages coronary artery disease may develop, leading to angina and myocardial infarction (heart attack) may occur.[2]
Classification
The diagnostic criteria for PXE are the typical skin biopsy appearance and the presence of angioid streaks in the retina. Other systems have become somewhat outdated by the discovery of the ABCC6 mutations.[2]
Pathophysiology
In PXE, there is mineralization (accumulation of calcium and other minerals) and fragmentation of the elastin-containing fibers in connective tissue, but primarily in the midlaminar layer of the dermis, Bruch's membrane and the midsized arteries.[4] Recent studies hypothesize that PXE is a metabolic disease, and that its features arise because metabolites of vitamin K cannot reach peripheral tissues.[5]
Genetics
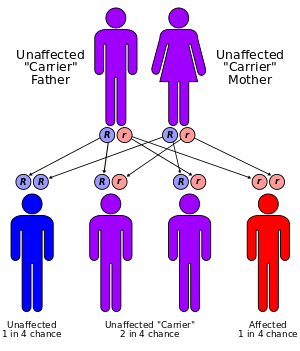
80% of clinical cases of pseudoxanthoma elasticum have detectable mutations in the ABCC6 gene.[6][7][8][9] Mutations in almost all parts of the gene have been described, of all types (missense, nonsense, splice alteration, insertion, small deletion or large deletion). Although there have been reports of autosomal dominant inheritance, the inheritance is typically autosomal recessive (both parents need to be carriers, and there is a 25% chance that a child will inherit both abnormal copies of the gene and therefore develop the condition).[2]
Strong genetic linkage was found with mutations in the ABCC6 gene, which codes for the MRP6 protein, but the exact mechanism by which this protein (which is a membrane transporter from the large ATP-binding cassette transporter family) influences the disease course is unknown; the protein is expressed in most organs, but mainly in the liver and kidney. It is unclear in what way this would lead to abnormalities in skin, eyes and blood vessels. It is thought that particular mutations do not cause a more severe or less severe form of the disease. Given the variations in age of onset and severity it is likely that other unknown risk factors (genetic and dietary) may be involved.[2] One study suggested that mutations causing total absence of an MRP6 protein caused a more severe disease,[10] but this could not be confirmed in a subsequent case series.[11]
Premature atherosclerosis is also associated with mutations in the ABCC6 gene, even in those without PXE.[12] A syndrome almost indistinguishable from hereditary PXE has been described in patients with hemoglobinopathies (sickle-cell disease and thalassemia) through a poorly understood mechanism.[2] In addition, there appears to be another PXE-like syndrome with a similar phenotype but as a result of problems with another gene, gamma-glutamyl carboxylase.[13]
Treatment
There is no treatment that directly interferes with the disease process, although dietary restriction of calcium has been tried with limited results.[2] For excessive areas of skin, plastic surgery may be needed. For the growth of abnormal blood vessels in the retina, laser photocoagulation and photodynamic therapy may be used; injections with triamcinolone have shown limited effect. Antiangiogenic drugs such as bevacizumab (Avastin) and ranibizumab (Lucentis) have been effective, similar to its efficacy in age-related macular degeneration.[3] Cardiovascular disease is treated as in individuals without PXE. Some recommend avoidance of nonsteroidal anti-inflammatory drugs (NSAIDS) that increase bleeding risk, such as aspirin, and ibuprofen.[2]
Epidemiology
The reported prevalence of pseudoxanthoma elasticum is about 1:25,000. Females are twice as likely to be affected as males. The disease occurs in all ethnicities, but Afrikaners are more likely to have PXE as a result of a founder effect (i.e. it was relatively prevalent in the small group of people from whom most Afrikaners descend).[2]
History
The first description of PXE that distinguished it from other xanthomatous conditions was by Dr Ferdinand-Jean Darrier in 1896.[14] The eponym "Grönblad-Strandberg syndrome" is used in older literature, after two physicians who made further discoveries in the disease manifestations.[15]
PXE has the distinction of being the only disease for which a layperson is the inventor of the gene, ABCC6. Sharon F. Terry, co-founder of PXE International with her husband, Patrick F. Terry, worked with scientists to discover and patent the gene in 2000.[8] The Terrys' two children have pseudoxanthoma elasticum.[16][17]
Images
 Pseudoxanthoma elasticum of the posterior lateral neck.
Pseudoxanthoma elasticum of the posterior lateral neck. Pseudoxanthoma elasticum of the left axillary fold.
Pseudoxanthoma elasticum of the left axillary fold.
See also
References
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- 1 2 3 4 5 6 7 8 9 10 11 12 Chassaing N, Martin L, Calvas P, Le Bert M, Hovnanian A (2005). "Pseudoxanthoma elasticum: a clinical, pathophysiological and genetic update including 11 novel ABCC6 mutations". J. Med. Genet. 42 (12): 881–92. doi:10.1136/jmg.2004.030171. PMC 1735972
 . PMID 15894595.
. PMID 15894595. - 1 2 3 Finger RP, Charbel Issa P, Ladewig MS, et al. (2009). "Pseudoxanthoma elasticum: genetics, clinical manifestations and therapeutic approaches". Surv Ophthalmol. 54 (2): 272–85. doi:10.1016/j.survophthal.2008.12.006. PMID 19298904.
- ↑ Gheduzzi D, Sammarco R, Quaglino D, Bercovitch L, Terry S, Taylor W, Ronchetti I (2003). "Extracutaneous ultrastructural alterations in pseudoxanthoma elasticum". Ultrastructural pathology. 27 (6): 375–84. doi:10.1080/716100800. PMID 14660276.
- ↑ Li Q, Jiang Q, Pfendner E, Váradi A, Uitto J (January 2009). "Pseudoxanthoma elasticum: clinical phenotypes, molecular genetics and putative pathomechanisms". Exp. Dermatol. 18 (1): 1–11. doi:10.1111/j.1600-0625.2008.00795.x. PMC 3349969. PMID 19054062.
- ↑ Ringpfeil F, Lebwohl MG, Christiano AM, Uitto J (2000). "Pseudoxanthoma elasticum: mutations in the MRP6 gene encoding a transmembrane ATP-binding cassette (ABC) transporter". Proc. Natl. Acad. Sci. U.S.A. 97 (11): 6001–6. doi:10.1073/pnas.100041297. PMC 18548. PMID 10811882.
- ↑ Bergen AA, Plomp AS, Schuurman EJ, et al. (2000). "Mutations in ABCC6 cause pseudoxanthoma elasticum". Nat. Genet. 25 (2): 228–31. doi:10.1038/76109. PMID 10835643.
- 1 2 Le Saux O, Urban Z, Tschuch C, et al. (2000). "Mutations in a gene encoding an ABC transporter cause pseudoxanthoma elasticum". Nat. Genet. 25 (2): 223–7. doi:10.1038/76102. PMID 10835642.
- ↑ Struk B, Cai L, Zäch S, et al. (2000). "Mutations of the gene encoding the transmembrane transporter protein ABC-C6 cause pseudoxanthoma elasticum". J. Mol. Med. 78 (5): 282–6. doi:10.1007/s001090000114. PMID 10954200.
- ↑ Schulz V, Hendig D, Szliska C, Götting C, Kleesiek K (2005). "Novel mutations in the ABCC6 gene of German patients with pseudoxanthoma elasticum". Hum. Biol. 77 (3): 367–84. doi:10.1353/hub.2005.0054. PMID 16392638.
- ↑ Pfendner EG, Vanakker OM, Terry SF, et al. (2007). "Mutation detection in the ABCC6 gene and genotype-phenotype analysis in a large international case series affected by pseudoxanthoma elasticum". J. Med. Genet. 44 (10): 621–8. doi:10.1136/jmg.2007.051094. PMC 2597973. PMID 17617515.
- ↑ Trip MD, Smulders YM, Wegman JJ, et al. (2002). "Frequent mutation in the ABCC6 gene (R1141X) is associated with a strong increase in the prevalence of coronary artery disease". Circulation. 106 (7): 773–5. doi:10.1161/01.CIR.0000028420.27813.C0. PMID 12176944.
- ↑ Vanakker OM, Martin L, Gheduzzi D, Leroy BP, Loeys BL, Guerci VI, Matthys D, Terry SF, Coucke PJ, Pasquali-Ronchetti I, De Paepe A (2007). "Pseudoxanthoma elasticum-like phenotype with cutis laxa and multiple coagulation factor deficiency represents a separate genetic entity". J Invest Dermatol. 127 (3): 581–7. doi:10.1038/sj.jid.5700610. PMID 17110937.
- ↑ Darrier FJ (1896). "Pseudoxanthoma elasticum". Monatschr Prakt Dermatol (in German). 23: 609–17.
- ↑ synd/1059 at Who Named It?
- ↑ Terry SF, Terry PF, Rauen KA, Uitto J, Bercovitch LG (2007). "Advocacy groups as research organizations: the PXE International example". Nat. Rev. Genet. 8 (2): 157–64. doi:10.1038/nrg1991. PMID 17230202.
- ↑ Terry SF (2003). "Learning genetics". Health Aff (Millwood). 22 (5): 166–71. doi:10.1377/hlthaff.22.5.166. PMID 14515892.
External links
- PXE International
- pxe at NIH/UW GeneTests
- Pseudoxanthoma elasticum at NLM Genetics Home Reference