Hypertensive emergency
| Malignant hypertension | |
|---|---|
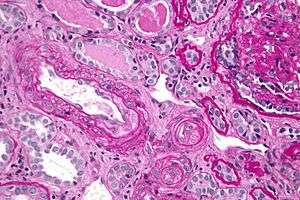 | |
| Micrograph showing thrombotic microangiopathy, a histomorphologic finding seen in malignant hypertension. Kidney biopsy. PAS stain. | |
| Classification and external resources | |
| Specialty | cardiology |
| ICD-10 | I10 |
| ICD-9-CM | 401-405 |
| DiseasesDB | 7788 |
| MedlinePlus | 000491 |
| eMedicine | article/241640 |
| Patient UK | Hypertensive emergency |
| MeSH | D006974 |
A hypertensive emergency (Systolic over 180 or diastolic over 120)(formerly called "malignant hypertension") is hypertension (high blood pressure) with acute impairment of one or more organ systems (especially the central nervous system, cardiovascular system and/or the renal system)[1] that can result in irreversible organ damage. In a hypertensive emergency, the blood pressure should be slowly lowered over a period of minutes to hours with an antihypertensive agent.
Signs and symptoms
The eyes may show retinal hemorrhage or an exudate. Papilledema must be present before a diagnosis of malignant hypertension can be made. The brain shows manifestations of increased intracranial pressure, such as headache, vomiting, and/or subarachnoid or cerebral hemorrhage. Patients will usually suffer from left ventricular dysfunction. The kidneys will be affected, resulting in hematuria, proteinuria, and acute renal failure. It differs from other complications of hypertension in that it is accompanied by papilledema.[2] This can be associated with hypertensive retinopathy.
Other signs and symptoms can include:
- Chest pain
- Arrhythmias
- Headache
- Epistaxis
- Dyspnea
- Faintness or vertigo
- Severe anxiety
- Agitation
- Altered mental status
- Paresthesias
- Vomiting
Chest pain requires immediate lowering of blood pressure (such as with sodium nitroprusside infusions), while urgencies can be treated with oral agents, with the goal of lowering the mean arterial pressure (MAP) by 20% in 1–2 days with further reduction to "normal" levels in weeks or months. The former use of oral nifedipine, a calcium channel blocker, has been strongly discouraged because it is not absorbed in a controlled and reproducible fashion and has led to serious and fatal hypotensive problems.
Sometimes, the term hypertensive emergency is also used as a generic term, comprising both hypertensive emergency, as a specific term for a serious and urgent condition of elevated blood pressure, and hypertensive urgency, as a specific term of a less serious and less urgent condition (the terminology hypertensive crisis is usually used in this sense).
Definition
| Terminology[3] | Systolic Pressure (mm Hg) | Diastolic Pressure (mm Hg) |
| Normal | < 120 | < 80 |
| Pre-hypertension | 120-139 | 80-89 |
| Hypertension stage 1 | 140-159 | 90-99 |
| Hypertension stage 2 | ≥ 160 | ≥ 100 |
| Hypertensive crisis - emergency | ≥ 180 | ≥ 120 |
The term hypertensive emergency is primarily used as a specific term for a hypertensive crisis with a diastolic blood pressure greater than or equal to 110 mmHg and/or systolic blood pressure greater than or equal to 180mmHg. Hypertensive emergency differs from hypertensive crisis in that, in the former, there is evidence of acute organ damage.
Causes
Many factors and causes are contributory in hypertensive crises. One main cause is the discontinuation of antihypertensive medications. Other common causes of hypertensive crises are autonomic hyperactivity, collagen-vascular diseases, drug use (particularly stimulants, especially cocaine and amphetamines and their substituted analogues), glomerulonephritis, head trauma, neoplasias, preeclampsia and eclampsia, and renovascular hypertension.[4]
During a hypertensive emergency uncontrolled blood pressure leads to progressive or impending end-organ dysfunction. Therefore, it is important to lower the blood pressure aggressively. Acute end-organ damage may occur, affecting the neurological, cardiovascular, renal, or other organ systems. Some examples of neurological damage include hypertensive encephalopathy, cerebral vascular accident/cerebral infarction, subarachnoid hemorrhage, and intracranial hemorrhage. Cardiovascular system damage can include myocardial ischemia/infarction, acute left ventricular dysfunction, acute pulmonary edema, and aortic dissection. Other end-organ damage can include acute renal failure or insufficiency, retinopathy, eclampsia, and microangiopathic hemolytic anemia.[5]
Extreme blood pressure can lead to problems in the eye, such as retinopathy or damage to the blood vessels in the eye.[6]
Pathophysiology
The pathophysiology of hypertensive emergency is not well understood.[7] Failure of normal autoregulation and an abrupt rise in systemic vascular resistance are typical initial components of the disease process.[8]
Hypertensive emergency pathophysiology includes:
- Abrupt increase in systemic vascular resistance, likely related to humoral vasoconstrictors
- Endothelial injury
- Fibrinoid necrosis of the arterioles
- Deposition of platelets and fibrin
- Breakdown of normal autoregulatory function
The resulting ischemia prompts further release of vasoactive substances, completing a vicious cycle. If the process is not stopped, a vicious cycle of homeostatic failure begins, leading to loss of cerebral and local autoregulation, organ system ischemia and dysfunction, and myocardial infarction.[9]
It is estimated that single-organ involvement is found in approximately 83% of hypertensive emergency patients, two-organ involvement in about 14% of patients, and multi-organ failure (failure of at least 3 organ systems) in about 3% of patients.
The most common clinical presentations of hypertensive emergencies are cerebral infarction (24.5%), pulmonary edema (22.5%), hypertensive encephalopathy (16.3%), and congestive heart failure (12%). Less common presentations include intracranial hemorrhage, aortic dissection, and eclampsia.[8]
Cerebral autoregulation is the ability of the blood vessels in the brain to maintain a constant blood flow. It has been shown that people who suffer from chronic hypertension can tolerate higher arterial pressure before their autoregulation system is disrupted. Hypertensives also have an increased cerebrovascular resistance which puts them at greater risk of developing cerebral ischemia if the blood flow decreases into a normotensive range. On the other hand, sudden or rapid rises in blood pressure may cause hyperperfusion and increased cerebral blood flow, causing increased intracranial pressure and cerebral edema. Hypertensive encephalopathy - characterized by hypertension, altered mentation, and papilledema- is one of the clinical manifestations of cerebral edema and microhemorrhages seen with dysfunction of cerebral autoregulation.[8]
Increased arterial stiffness, increased systolic blood pressure, and widened pulse pressures, all resulting from chronic hypertension, can lead to heart damage. Coronary perfusion pressures are decreased by these factors, which also increase myocardial oxygen consumption, possibly leading to left ventricular hypertrophy. As the left ventricle becomes unable to compensate for an acute rise in systemic vascular resistance, left ventricular failure and pulmonary edema or myocardial ischemia may occur.
Chronic hypertension has a great impact on the renal vasculature, leading to pathologic changes in the small arteries of the kidney. Affected arteries develop endothelial dysfunction and impairment of normal vasodilation, which alter renal autoregulation. When the renal autoregulatory system is disrupted, the intraglomerular pressure starts to vary directly with the systemic arterial pressure, thus offering no protection to the kidney during blood pressure fluctuations. During a hypertensive crisis, this can lead to acute renal ischemia.
Endothelial injury can occur as a consequence of severe elevations in blood pressure, with fibrinoid necrosis of the arterioles following. The vascular injury leads to deposition of platelets and fibrin, and a breakdown of the normal autoregulatory function. Ischemia occurs as a result, prompting further release of vasoactive substances. This process completes the vicious cycle.[4]
Treatment
Several classes of antihypertensive agents are recommended, with the choice depending on the etiology of the hypertensive crisis, the severity of the elevation in blood pressure, and the usual blood pressure of the patient before the hypertensive crisis. In most cases, the administration of an intravenous sodium nitroprusside injection, which has an almost immediate antihypertensive effect, is suitable (but in many cases not readily available). In less urgent cases, oral agents like captopril, clonidine, labetalol, or prazosin can be used, but all have a delayed onset of action (by several minutes) compared to sodium nitroprusside. Controlled bloodletting is an effective salvage therapy in the interim when nitroprusside is unavailable, and aggressive oral therapy has not yet taken effect.
In addition, non-pharmacological treatment could be considered in cases of resistant malignant hypertension due to end stage renal failure, such as: surgical nephrectomy, laparoscopic nephrectomy and renal artery embolization in cases of anesthesia risk.[10]
It is also important that the blood pressure be lowered smoothly, not too abruptly. The initial goal in hypertensive emergencies is to reduce the pressure by no more than 25% (within minutes to 1 or 2 hours), and then toward a level of 160/100 mm Hg within a total of 2–6 hours. Excessive reduction in blood pressure can precipitate coronary, cerebral, or renal ischemia and, possibly, infarction.[11]
The diagnosis of a hypertensive emergency is not based solely on an absolute level of blood pressure, but also on the typical blood pressure level of the patient before the hypertensive crisis occurs. Individuals with a history of chronic hypertension may not tolerate a "normal" blood pressure.
Epidemiology
Although an estimated 50 million or more adult Americans suffer from hypertension, the relative incidence of hypertensive crisis is relatively low (less than 1% annually). Nevertheless, this condition does affect upward of 500,000 Americans each year, and is therefore a significant cause of serious morbidity in the US.[12]
According to a research published in 2006, hypertension prevalence is again on the rise, with 28.6% of the U.S. population estimated to be suffering from it in the period 1999-2002. According to the study, relative incidence rates of hypertension range between 3% and 18% of the population. These numbers depend on the age, gender, ethnicity, and body size.[13]
According to Whelton, the incidence and prevalence of hypertension is about 50% higher in African-American adults than in white or Mexican-American populations. Also, Whelton adds that prevalence of hypertension has increased progressively in children and adolescents between 1988-2000. According to this study, recent estimates indicate that approximately 1 billion adults worldwide have hypertension, with the highest prevalence of hypertension in Eastern Europe and the Latin American/Caribbean region.[14]
As a result of the use of antihypertensives, the incidence of hypertensive emergencies has declined from 7% to 1% of patients with hypertension. The 1–year survival rate has also increased. Before 1950, this survival rate was only 20%, but it is now more than 90% with proper medical treatment.[8]
Estimates indicate that approximately 1% to 2% of patients with hypertension develop hypertensive crisis at some point in their lifetime. Men are more commonly affected by hypertensive crises than women.
The incidence of hypertensive crises has increased and hospital admissions tripled between 1983 and 1990, from 23,000 to 73,000 per year in the United States. The incidence of postoperative hypertensive crisis varies and such variation depends on the population examined. Most studies report and incidence of between 4% to 35%.[15]
Prognosis
Severe hypertension is a serious and potentially life-threatening medical condition. It is estimated that people who do not receive appropriate treatment only live an average of about three years after the event.[16]
The morbidity and mortality of hypertensive emergencies depend on the extent of end-organ dysfunction at the time of presentation and the degree to which blood pressure is controlled afterward. With good blood pressure control and medication compliance, the 10-year survival rate of patients with hypertensive crises approaches 70%.[17]
The risks of developing a life-threatening disease affecting the heart or brain increase as the blood flow increases. Commonly, ischemic heart attack and stroke are the causes that lead to death in patients with severe hypertension. It is estimated that for every 20 mm Hg systolic or 10 mm Hg diastolic increase in blood pressures above 115/75 mm Hg, the mortality rate for both ischemic heart disease and stroke doubles.
Several studies have concluded that African Americans have a greater incidence of hypertension and a greater morbidity and mortality from hypertensive disease than non-Hispanic whites.[18] It appears that hypertensive crisis is also more common in African Americans compared with other races.
Although severe hypertension is more common in the elderly, it may occur in children (though very rarely). Also, women have slightly increased risks of developing hypertension crises than do men. The lifetime risk for developing hypertension is 86-90% in females and 81-83% in males.
See also
References
- ↑ Thomas L (October 2011). "Managing hypertensive emergencies in the ED". Can Fam Physician. 57 (10): 1137–97. PMC 3192077
 . PMID 21998228.
. PMID 21998228. - ↑ "malignant hypertension" at Dorland's Medical Dictionary
- ↑ Chobanian et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 Report. JAMA 2003; ;289(19):2560-2571. doi:10.1001/jama.289.19.2560
- 1 2 "Hypertensive Crises: Recognition and Management". Retrieved 2010-07-27.
- ↑ "Hypertension -pathophysiology". Retrieved 2010-07-27.
- ↑ "Blurred Vision Causes". Retrieved 2010-07-27.
- ↑ "Hypertensive Emergencies". Retrieved 2010-04-20.
- 1 2 3 4 "Pathophysiology". Retrieved 2010-04-20.
- ↑ "Vascular Biology Working Group". Retrieved 2010-04-20.
- ↑ http://www.avicennajmed.com/article.asp?issn=2231-0770;year=2013;volume=3;issue=1;spage=23;epage=25;aulast=Alhamid;type=0
- ↑ Brewster LM, MD; Michael Sutters, MD (2006). "Hypertensive Urgencies & Emergencies - Hypertension Drug Therapy". Systemic Hypertension. Armenian Health Network, Health.am. Retrieved 2007-12-02.
- ↑ Vidt DG (2001). "Emergency room management of hypertensive urgencies and emergencies". Cleveland Clinic Foundation. Retrieved 2007-12-02.
- ↑ "Hypertension: Trends in Prevalence, Incidence, and Control". Retrieved 2010-07-27.
- ↑ "Prevalence and Incidence of Hypertension". Retrieved 2010-07-27.
- ↑ "Hypertensive Crises" (PDF). Retrieved 2010-07-27.
- ↑ "Severe Hypertension Symptoms". Retrieved 2010-04-20.
- ↑ "Mortality/Morbidity". Retrieved 2010-04-20.
- ↑ Howard, J. (1965). "Race Differences in Hypertension Mortality Trends: Differential Drug Exposure as a Theory". Systemic Hypertension. Milbank Mem Fund Q. 43: 202–218. JSTOR 3349030.