Fuchs' dystrophy
| Fuchs' dystrophy | |
|---|---|
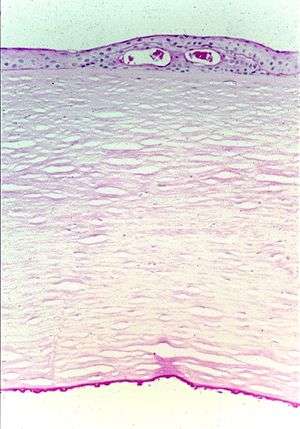 | |
| Fuchs' corneal dystrophy. Light microscopic appearance of the cornea showing numerous excrescences (guttae) on the posterior surface of Descemet's membrane and the presence of cysts in the corneal epithelium beneath ectopically placed intraepithelial basement membrane. Periodic acid-Schiff stain. From a review by Klintworth, 2009.[1] | |
| Classification and external resources | |
| Specialty | ophthalmology |
| ICD-10 | H18.5 |
| ICD-9-CM | 371.57 |
| OMIM | 136800 610158 |
| DiseasesDB | 31163 |
| MedlinePlus | 007295 |
| eMedicine | article/1193591 |
| MeSH | D005642 |
Fuchs' dystrophy (pronounced fooks-DIS-trə-fe), also known as Fuchs' corneal endothelial dystrophy or FCED, is a slowly progressing corneal dystrophy that usually affects both eyes and is slightly more common in women than in men. Although doctors can often see early signs of Fuchs' dystrophy in people in their 30s and 40s, the disease rarely affects vision until people reach their 50s and 60s.
The condition was first described by Austrian ophthalmologist Ernst Fuchs (1851–1930), after whom it is named. In 1910, Fuchs first reported 13 cases of central corneal clouding, loss of corneal sensation and the formation of epithelial bullae, which he labeled ‘dystrophia epithelialis corneae’. It was characterized by late onset, slow progression, decreased visual acuity in the morning, lack of inflammation, diffuse corneal opacity, intense centrally, and roughened epithelium with vesicle-like features.[2] A shift to the understanding of Fuchs’ corneal endothelial dystrophy (FCED) as primarily a disease of the corneal endothelium resulted after a number of observations in the 1920s. Crystal-like features of the endothelium were noted by Kraupa in 1920, who suggested that the epithelial changes were dependent on the endothelium. Using a slit lamp, Vogt described the excrescences associated with FCD as drop-like in appearance in 1921. In 1924, Graves then provided an extremely detailed explanation of the endothelial elevations visible with slit-lamp biomicroscopy. A patient with unilateral epithelial dystrophy and bilateral endothelial changes was described by the Friedenwalds in 1925; subsequent involvement of the second eye led them to emphasize that endothelial changes preceded epithelial changes. As only a subset of patients with endothelial changes proceeded to epithelial involvement, Graves stated on 19 October 1925 to the New York Academy of Medicine that “Fuchs’ epithelial dystrophy may be a very late sequel to severer cases of the deeper affection”.[3]
Epidemiology
Few studies have examined the prevalence of FCED on a large scale. First assessed in a clinical setting, Fuchs himself estimated the occurrence of dystrophia epithelialis corneae to be one in every 2000 patients; a rate that is likely reflective of those who progress to advanced disease. Cross-sectional studies suggest a relatively higher prevalence of disease in European countries relative to other areas of the world. Fuchs' dystrophy rarely affects individuals under 50 years of age.[4]
Etiology
Fuchs’ corneal endothelial dystrophy (FCED) is a degenerative disease of the corneal endothelium with accumulation of focal outgrowths called guttae (drops) and thickening of Descemet’s membrane, leading to corneal edema and loss of vision. The corneal endothelial cell layer and its basement membrane (Descemet's membrane) acts as a barrier to hydration of the corneal stroma by aqueous humor and are “pump” cells of the cornea that function to maintain hydration of the cornea at a specific level that maintains corneal stromal clarity through precise spatial arrangement of collagen fibers. In FED, Descemet’s membrane is grossly thickened with accumulation of abnormal wide-spaced collagen and numerous guttae. Corneal endothelial cells in end-stage FED are reduced in number and appear attenuated, causing progressive stromal edema (swelling). Progressive endothelial cell loss causes relative influx of aqueous humor into the cornea, leading to swelling (corneal stromal edema), which results in blurred vision. Eventually, the epithelium also becomes edematous, resulting in more severe visual impairment. Focal blisters of epithelial edema ("bullae") may be particularly painful when they burst.
The inheritance of FCED is complex and polymorphic such that although inheritance is autosomal dominant there are genetic and environmental modifiers that determine the degree to which member of the same family express the disease. There is reasonable evidence of associations between transcription factor 4 (TCF4) genetic polymorphisms and risk of Fuchs' endothelial dystrophy (FED).[5] Endothelial cell loss may be aggravated or accelerated by intraocular trauma or surgery. A common scenario involves prolonged corneal swelling or edema following cataract surgery or other types of ocular surgery. Hence, patients with a history of Fuchs' dystrophy may be at a greater risk of corneal edema after ocular surgery as they have fewer functioning endothelial cells.
FCED is classified into 4 stages, from early signs of guttae formation to end-stage subepithelial scarring. Diagnosis is made by biomicroscopic examination in the clinic. Other modalities, such as corneal thickness measurement (pachymetry), in-vivo confocal biomicroscopy, and specular microscopy can be used in conjunction.
Exact pathogenesis is unknown but factors include endothelial cell apoptosis, sex hormones, inflammation, and aqueous humor flow and composition. Mutations in collagen VIII, a major component of Descemet’s membrane secreted by endothelial cells, have been linked to the early-onset FCED.[6]
Genes include:
| Type | OMIM | Gene | Locus |
|---|---|---|---|
| FECD1 | 136800 | COL8A2 | 1p34.3-p32.3 |
| FECD4 | 610206 | SLC4A11 | 20p13-p12 |
| FECD6 | 189909 | ZEB1 | 10p11.2 |
Signs and symptoms
FED may be discovered as an incidental finding at a routine optometrist visit or by an ophthalmologist during assessment for cataract surgery. As a result of irregularities on the inner surface of the cornea affected individuals may simply notice a reduction in the quality of vision or glare or haloes particularly when driving at night. Individuals with symptomatic Fuchs' dystrophy typically awaken with blurred vision which improves during the day.[4] This occurs because the cornea is normally more swollen in the morning due to nocturnal fluid retention in the absence of normal evaporation due to the lids being closed. During waking hours this fluid evaporates once the eyes are open. As the disease worsens vision remains blurred despite evaporation due to endothelial pump failure and fluid retention. As Fuchs' dystrophy typically occurs in older individuals there may also be cataract of the lens which will also reduce vision.
Researchers are finding that Fuchs' is a genetically heterogeneous disease, and many different genes and loci have been associated as contributing to a small percentage of overall Fuchs' cases. Certain genetic lesions have been correlated with more severe disease and earlier onset.[7][8][9] Therefore, some individuals may experience symptoms of the disease at a much earlier age, while others may not experience symptoms until late in life.
Treatment
Non-surgical treatments of FCED may be used to treat symptoms of early disease. Medical management includes topical hypertonic saline, the use of a hairdryer to dehydrate the precorneal tear film, and therapeutic soft contact lenses. Hypertonic saline draws water out of the cornea through osmosis. When using a hairdryer, the patient is instructed to hold it at an arm's length or directed across the face on a cold setting, to dry out the epithelial blisters. This can be done two or three times a day. Definitive treatment, however, (especially with increased corneal edema) is surgical in the form of corneal transplantation.
Globall, full thickness corneal grafts (penetrating keratoplasty - PKP) remain the most widely practiced form of corneal transplantation. Since 1998, new surgical modalities in the treatment of FCED have been developed, initially by G. Melles et al. in The Netherlands. These procedures, called posterior lamellar keratoplasty or endothelial keratoplasty, were initially popularized as deep lamellar endothelial keratoplasty (DLEK) and then evolved to Descemet’s stripping endothelial keratoplasty (DSEK)/ Descemet’s stripping automated endothelial keratoplasty (DSAEK) and more recently Descemet's membrane endothelial keratoplasty (DMEK). DSEK and DMEK avoid some of the surgical complications of PKP such as wound dehiscence and high postoperative astigmatism but are technically more demanding and require specialist training of the surgeon.
Improved surgical instrumentation for DSEK, such as donor graft injectors, and technical improvements in the surgical technique have facilitated reduced complications and the potential to perform DSEK through small incisions. These key technical improvements are primarily aimed at allowing graft insertion whilst causing the least possible damage to donor endothelial cells, thereby delivering the greatest load of fully functional endothelial cells into the patient's eye. In DSAEK a very thin layer of cornea including endothelial cells is attached onto the inner surface of the patient's cornea. This cell layer is initially maintained in position by filling the anterior chamber of the eye with a bubble of air which is subsequently reabsorbed by the body.[10]
Descemet Membrane Endothelial Keratoplasty (DMEK) is perhaps the purest form of endothelial transplantation. In DMEK only a donor Descemet membrane and its endothelium is transplanted into the recipient. Following DMEK, 90% of cases achieve a best spectacle corrected visual acuity 20/40 or better, and 60% of cases 20/25 or better within 1–3 months, although complications such as graft failure and detachment remain challenges for the patient and surgeon. DMEK Surgery can be technically challenging as the cell layer has a tendency to scroll in the aqueous of the anterior chamber and requires careful manipulation to unfold and centre (video ). The surgeon needs to do this without touching the scroll to avoid damaging the transplanted cells. DMEK is reported to have the lowest rejection rate of any type of endothelial cell graft.[11] DMEK has now superseded DSEK as the procedure of choice for pure endothelial cells dysfunctions such as Fuchs' Dystrophy in specialist centres.
Cataract is often present in patients with Fuchs' Dystrophy. Cataract surgery alone can exacerbate corneal swelling due to further endothelial cell loss. Specialist surgeons will often combine cataract surgery with DSEK/DMEK at the same time.
More speculative future directions in the treatment of FED include in-vitro expansion of human corneal endothelial cells for transplantation, artificial corneas (keratoprosthesis) and genetic modification. No graft surgery where the central diseased endothelium is stripped off but not replaced with donor tissue has also shown some promise in selected patients. Visual recovery is thought to occur due to peripheral endothelial cell migration into the denuded area of cells. What is very promising is the effect of Rho Kinase (ROCK) inhibition on endothelial cell division and proliferation. ROCK inhibition may offer a viable medical treatment or cell therapy for Fuchs Endothelial Dystrophy within the next decade.[12]
A greater understanding of FED pathophysiology may assist in future with the development of treatments to prevent progression of disease. Although much progress has been made in the research and treatment of FED, many questions remain to be answered. The exact causes of illness, the prediction of disease progression and delivery of an accurate prognosis, methods of prevention and effective nonsurgical treatment are all the subject of inquiries that necessitate an answer. Increased attention must be given to research that can address the most basic questions of how the disease develops: what are the biomolecular pathways implicated in disease, and what genetic or environmental factors contribute to its progression? In addition to shaping our understanding of FED, identification of these factors would be essential for the prevention and management of this condition.[3]
See also
- Fuchs heterochromic iridocyclitis (a disease of the iris)
- Ocular straylight
References
- ↑ Klintworth GK (2009). "Corneal dystrophies". Orphanet J Rare Dis. 4 (1): 7. doi:10.1186/1750-1172-4-7. PMC 2695576
 . PMID 19236704.
. PMID 19236704. - ↑ Fuchs E. Dystrophia epithelialis corneae. Graefes Arch Clin Exp Ophthalmol. 1910:478–508.
- 1 2 Eghrari, Allen O; John D Gottsch (April 2010). "Fuchs' corneal dystrophy". Expert Rev Ophthalmol. 5 (2): 147–159. doi:10.1586/eop.10.8. PMC 2897712. PMID 20625449.
- 1 2 Kunimoto, Derek; Kunal Kanitkar; Mary Makar (2004). The Wills eye manual: office and emergency room diagnosis and treatment of eye disease. (4th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. pp. 80–80. ISBN 978-0781742078.
- ↑ Li, Dan; Peng, XiaoYan; Sun, HuiYu (2015-01-01). "Association of TCF4 polymorphisms and Fuchs' endothelial dystrophy: a meta-analysis". BMC ophthalmology. 15: 61. doi:10.1186/s12886-015-0055-6. ISSN 1471-2415. PMC 4474332. PMID 26087656.
- ↑ Gottsch JD, Sundin OH, Liu SH, et al. (June 2005). "Inheritance of a novel COL8A2 mutation defines a distinct early-onset subtype of fuchs corneal dystrophy". Invest. Ophthalmol. Vis. Sci. 46 (6): 1934–9. doi:10.1167/iovs.04-0937. PMID 15914606.
- ↑ Eghrari, AO; McGlumphy, EJ; Iliff, BW; Wang, J; Emmert, D; Riazuddin, SA; Katsanis, N; Gottsch, JD (June 2012). "Prevalence and severity of fuchs corneal dystrophy in Tangier Island.". American journal of ophthalmology. 153 (6): 1067–72. doi:10.1016/j.ajo.2011.11.033. PMID 22321803.
- ↑ Meadows, DN; Eghrari, AO; Riazuddin, SA; Emmert, DG; Katsanis, N; Gottsch, JD (December 2009). "Progression of Fuchs corneal dystrophy in a family linked to the FCD1 locus.". Investigative Ophthalmology & Visual Science. 50 (12): 5662–6. doi:10.1167/iovs.09-3568. PMID 19608546.
- ↑ McGlumphy, EJ; Yeo, WS; Riazuddin, SA; Al-Saif, A; Wang, J; Eghrari, AO; Meadows, DN; Emmert, DG; Katsanis, N; Gottsch, JD (December 2010). "Age-severity relationships in families linked to FCD2 with retroillumination photography.". Investigative Ophthalmology & Visual Science. 51 (12): 6298–302. doi:10.1167/iovs.10-5187. PMC 3055756. PMID 20811064.
- ↑ Bhogal, Maninder S.; Angunawela, Romesh I.; Bilotti, Emiliano; Eames, Ian; Allan, Bruce D. (2012-06-01). "Theoretical, experimental, and optical coherence tomography (OCT) studies of graft apposition and adhesion in Descemets stripping automated endothelial keratoplasty (DSAEK)". Investigative Ophthalmology & Visual Science. 53 (7): 3839–3846. doi:10.1167/iovs.12-9593. ISSN 1552-5783. PMID 22427600.
- ↑ Price, Marianne O.; Price, Francis W.; Kruse, Friedrich E.; Bachmann, Bjöern O.; Tourtas, Theofilos (2014-09-01). "Randomized comparison of topical prednisolone acetate 1% versus fluorometholone 0.1% in the first year after descemet membrane endothelial keratoplasty". Cornea. 33 (9): 880–886. doi:10.1097/ICO.0000000000000206. ISSN 1536-4798. PMID 25062336.
- ↑ Okumura, Naoki; Sakamoto, Yuji; Fujii, Keita; Kitano, Junji; Nakano, Shinichiro; Tsujimoto, Yuki; Nakamura, Shin-Ichiro; Ueno, Morio; Hagiya, Michio (2016-01-01). "Rho kinase inhibitor enables cell-based therapy for corneal endothelial dysfunction". Scientific Reports. 6: 26113. doi:10.1038/srep26113. ISSN 2045-2322. PMC 4870691. PMID 27189516.
External links
- Facts About the Cornea and Corneal Disease - The National Eye Institute (United States)
- Fuchs' dystrophy at DMOZ