Camptodactyly
| Camptodactyly | |
|---|---|
| Classification and external resources | |
| Specialty | medical genetics |
| ICD-10 | Q68.1 |
| ICD-9-CM | 755.59 |
| OMIM | 114200 |
| DiseasesDB | 30760 |
Camptodactyly is a medical condition that causes one or more fingers to be permanently bent. It involves fixed flexion deformity of the proximal interphalangeal joints. The fifth finger is always affected.
Camptodactyly can be caused by a genetic disorder. In that case, it is an autosomal dominant trait that is known for its incomplete genetic expressivity. This means that when a person has the genes for it, the condition may appear in both hands, one, or neither. A linkage scan proposed that the chromosomal locus of camptodactyly was 3q11.2-q13.12.[1]
Etymology
The name is derived from the ancient Greek words kamptos (bent) and daktylos (finger).
Causes
The specific cause of camptodactyly remains unknown, but there are a few deficiencies that lead to the condition. A deficient lumbrical controlling the flexion of the fingers, and abnormalities of the flexor and extensor tendons.[2]
A number of congenital syndromes may also cause camptodactyly:
- Jacobsen syndrome
- Beals Syndrome [3]
- Blau syndrome
- Freeman-Sheldon syndrome
- Cerebrohepatorenal syndrome
- Weaver syndrome
- Christian syndrome 1
- Gordon Syndrome
- Jacobs arthropathy-camptodactyly syndrome
- Lenz microphthalmia syndrome
- Marshall-Smith-Weaver syndrome
- Oculo-dento-digital syndrome
- Tel Hashomer camptodactyly syndrome
- Toriello-Carey syndrome
- Stuve-Wiedemann syndrome
- Loeys-Dietz syndrome
- Fryns syndrome[4]
- Marfan's syndrome[5]
- Carnio-carpo-tarsal dysthropy[5]
Pattern of inheritance
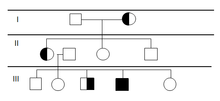
The pattern of inheritance is determined by the phenotypic expression of a gene—which is called expressivity.[6] Camptodactyly can be passed on through generations in various levels of phenotypic expression, which include both or only one hand. This means that the genetic expressivity is incomplete. It can be inherited from either parent.
In most of its cases, camptodactyly occurs sporadically, but it has been found in several studies that it is inherited as an autosomal dominant condition.[1]
Treatment

If a contracture is less than 30 degrees, it may not interfere with normal functioning.[2] The common treatment is splinting and occupational therapy.[7] Surgery is the last option for most cases as the result may not be satisfactory.[8]
See also
References
- 1 2 Malik, Sajid; Jörg Schott; Julia Schiller; Anna Junge; Erika Baum; Manuela C Koch (2008). "Fifth finger camptodactyly maps to chromosome 3q11.2–q13.12 in a large German kindred.". European Journal of Human Genetics 2. 16 (2): 265. doi:10.1038/sj.ejhg.5201957.
- 1 2 Kozin, Scott H. (2004). Hand Surgery. Lippincott Williams & Wilkins.
- ↑ Callewaert, B. L.; Loeys, B. L.; Ficcadenti, A; Vermeer, S; Landgren, M; Kroes, H. Y.; Yaron, Y; Pope, M; Foulds, N; Boute, O; Galán, F; Kingston, H; Van Der Aa, N; Salcedo, I; Swinkels, M. E.; Wallgren-Pettersson, C; Gabrielli, O; De Backer, J; Coucke, P. J.; De Paepe, A. M. (2009). "Comprehensive clinical and molecular assessment of 32 probands with congenital contractural arachnodactyly: Report of 14 novel mutations and review of the literature". Human Mutation. 30 (3): 334–41. doi:10.1002/humu.20854. PMID 19006240.
- ↑ Young I. D.; Simpson K.; Winter R. M. (1986). "A case of Fryns syndrome". J. Med. Genet. 23 (1): 82–88. doi:10.1136/jmg.23.1.82. PMC 1049547
 . PMID 3950939.
. PMID 3950939. - 1 2 Metin Işık (2011). Turkish Journal of Physical Medicine and Rehabilitation http://www.ftrdergisi.com/tr/makale/1836/178/Tam-Metin. Retrieved 11/3/2013. Check date values in:
|access-date=(help); Missing or empty|title=(help) - ↑ Cummings, Michael R. (2011). Human Heredity: Principles and Issues. Cengage Learning. pp. 87, 88.
- ↑ http://childrenshospital.org/az/Site644/mainpageS644P4.html
- ↑ http://congenitalhand.wustl.edu/2012/03/camptodactyly.html
External links
| Wikimedia Commons has media related to Camptodactyly. |
- http://www.childrenshospital.org/az/Site644/mainpageS644P0.html
- http://medind.nic.in/maa/t04/i3/maat04i3p227.pdf